Tout sur les médicaments הכל על תרופות كل شيئ عن الأدوية Все о наркотиках 关于药品的一切 డ్రగ్స్ గురించి అన్ని 마약에 관한 모든 것 Όλα για τα Ναρκωτικά Complete Tracking of Drugs Across the World by Dr Anthony Melvin Crasto, Worldpeacepeaker, worlddrugtracker, PH.D (ICT), MUMBAI, INDIA, Worlddrugtracker, Helping millions, 9 million hits on google on all websites, 2.5 lakh connections on all networks, “ALL FOR DRUGS” CATERS TO EDUCATION GLOBALLY, No commercial exploits are done or advertisements added by me. This is a compilation for educational purposes only. P.S. : The views expressed are my personal and in no-way suggest the views of the professional body or the company that I represent
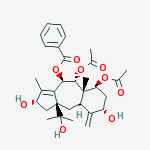
Brevifoliol was first isolated from the leaves of the plant Taxus brevifolia (F. Balza et al Phytochemistry 30, p. 1613-1614 (1991)). The process of its isolation involved extracting the fresh leaves of Taxus wallichiana with ethyl alcohol to get an extract. The crude extract after concentration was diluted with water and partitioned between hexane, chloroform and ethyl acetate sequentially. The chloroform extract upon concentration yielded a dark brown residue. The resultant residue was subjected to column chromatography over silica gel and eluted with chloroform and chloroform-methanol gradient. Six fractions were collected and brevifoliol was isolated from fraction five by rechromatography over silica gel and eluting with hexane-ethyl acetate gradient.
Brevifoliol has been isolated from other species of Taxus including the Himalayan yew Taxus wallichiana which is available in India., Recently, the structure of brevifoliol has been revised and it was shown to belong to 11 (15→1) abeo taxoid bicyclic skeleton of formula (1). The isolation of brevifoliol from leaves of the plantTaxus wallichiana is also reported in S. K. Chattopadhyay et al Indian J. Chemistry 35B, 175-177(1996) as part of studies on the isolation of anticancer compounds. The process of this disclosure involved extracting the dried and crushed needles of Taxus wallichiana with methanol for 72 hours and the extract was concentrated in vacuo. The concentrate was diluted with water and extracted with hexane and chloroform respectively. Concentration of the chloroform phase under vacuum left a residue which was separated by column chromatography over silica gel. Fraction eluted with chloroform-methanol (98:5) contained brevifoliol which was further purified by re-chromatography over silica gel and eluted with chloroform-methanol (99:2). Fractions containing brevifoliol were combined and concentrated and recrystallized from pet-ether and ethyl acetate mixture to get brevifoliol as needles. In in vitro testing of brevifoliol, it was found to have significant anticancer activity against different cancer cell lines. The detection of anticancer activity in brevifoliol prompted the present investigators to develop an efficient processing technology for isolation of the compound in large quantities from the needles of the plant for further biological testing.
The prior art process of isolation of brevifoliol suffers from a number of disadvantages including partitioning of the aqueous extract with hexane and chloroform and repeated column chromatography to get the compound. Although the partitioning of the aqueous phase with organic solvents works on small scale, it forms thick emulsions on large scale partitioning process and creates hindrance in getting the fractions separated. Also, the use of repeated chromatography might be useful on small-scale isolation of brevifoliol, it is only cumbersome, tedious and not economical on large-scale process.
Assignee: Council of Scientific and Industrial Research, New Delhi, India
Title or Subject: Process for Preparing Brevifoliol
Brevifoliol is found in the leaves of the plants of the genus Taxus and is useful as an anticancer agent. This patent describes a method of extracting from the leaves of the plantTaxus wallichiana (Tw) Alternative methods are known for extracting from Tw but they are said to suffer from several disadvantages. These include partitioning of an aqueous extract with hexane and CHCl3 and the repeated use of chromatography to obtain the purified compound. The partitioning is said to work well on a small scale, but on a large scale thick emulsions are formed. Hence, the objective of the work in this patent is to provide a process that can be operated on a large scale. The process developed comprises the following steps:
(i) Dry and pulverize the leaves of the plant.
(ii) Extract the dried leaves with an alcohol such as MeOH or EtOH at 20−40 °C over 3 days.
(iii) Concentrate the alcoholic solution and adsorb the extract onto Celite.
(iv) Dry the Celite adsorbate at 20−50 °C for up to 48 h.
(v) Extract the dried adsorbate with 60−80 petroleum ether then CHCl3 and concentrate the CHCl3 extract.
(vi) Subject the concentrated mixture to gross fractionation over a column of silica gel using CHCl3 add 2% MeOH in CHCl3.
(vii) Subject the later eluate to further chromatography over alumina in petroleum ether using 10% EtOAc in petroleum ether.
(viii) Recrystallise from EtOAc/petroleum ether as needles.
Brevifoliol
Advantages
The patent claims that the solvents can be recycled so that the process is cost-effective. Certainly it is true that avoiding water removes the emulsification problem, but two chromatographic steps are involved, and the use of so many solvents would seem to create handling problems on a commercial plant.
MONTELUKAST (Singulair® Oral Granules) helps to reduce asthma symptoms (coughing, wheezing, shortness of breath, or chest tightness) and control your asthma. It does not provide instant relief and cannot be used to treat a sudden asthma attack. It works only when used on a regular basis to help reduce inflammation and prevent asthma attacks. This drug is also helpful in improving seasonal allergies, like hay fever. Montelukast is effective in adults and children
Amongst the US approvals, tentative FDA approvals have been identified for generic Montelukast sodium, awarded to Endo, Glenmark, Mylan, Roxane, Sandoz, Teva and Torrent. The large number of generic authorisations awaiting launch in the UK is indicative of the likely competition the Singulair product will face across Europe upon SPC expiry
EP Pat. No. 480,717 discloses Montelukast sodium along with other related compounds and the methods for their preparation. The reported method of synthesis proceeds through corresponding methyl ester namely, Methyl 2-[(3S)-[3-[(2E)-(7-chloroquinolin – 2yl) ethenyl] phenyl] – 3 – hydroxypropyl] benzoate and involves coupling methyl 1- (mercaptomethyi) cyclopropaneacetate with a mesylate generated in-situ. The methyl ester of Montelukast is hydrolyzed to free acids and the latter converted directly to Montelukast Sodium salt (Scheme -1). The process is not particularly suitable for large – scale production because it requires tedious chromatographic purification of the methyl ester intermediate and / or the final product and the product yield is low.
Scheme -1
U.S. Pat. No. 5,614632 disclosed a process for the preparation of crystalline Montelukast sodium, which comprises of the following steps (Scheme – 2):
■ Reaction of methyl 2-[3(S)-[3-[2-(7-chloroquinolin -2-yl) ethenyl] phenyl] -3- hydroxypropyl benzoate (I) with Grignard reagent, methyl magnesium chloride in presence of cerium chloride to give Diol (II) ■ Reaction of Diol (II) with methane sulfonyl chloride to afford 2-[2-[3 (s)-[3- (2-(7-chloro quinolin-2yl) ethenyl] phenyl]- 3 – methane sulfonyloxy propyl] phenyl] -2-propanol (III)
■ Condensation of 2-[2-[3(s)-[3-(2-(7-chloro quinolin – 2-yl) ethenyl] phenyl] –
3 – methane sulfonyloxypropyl] phenyl] – 2- propanol (III) with dilithium anion of 1-mercaptomethyl) cyclopropaneacetic acid, which has been generated by the reaction of l-(mercaptomethyl)cyclopropaneacetic acid (IV)with n-Butyl lithium
■ Isolation of the condensed product, Montelukast as solid Montelukast dicyclohexylamine salt
■ Purification and conversion of Montelukast dicyclohexylamine salt into Montelukast sodium
■ Crystallization of Montelukast sodium from a mixture of toluene and acetonitrile
The process disclosed in U.S Pat. No. 5,614,632 further involved the reaction of Diol (II) with methane sulfonyl chloride involves the reaction temperature of about – 25°C and the storage condition of the intermediate, 2-[2-[3(s)-[3-(2-(7-chloro quinolin – 2-yl) ethenyl] pheny] -3 -methane sulfonyloxy propyl] phenyl] -2-propanol (III) at temperature below – 150C for having the stability. The process further involves the reaction, formation of dilithium anion of l-(mercaptomethyl) cyclopropaneacetic acid which requires the usage of n-Butyl lithium, a highly flammable and hazardous reagent and the reaction is at temperature below -5°C further requires anhydrous conditions. Scheme – 2
Montelukast (trade names Singulair, Montelo-10, and Monteflo and Lukotas in India) is a leukotriene receptor antagonist(LTRA) used for the maintenance treatment of asthma and to relieve symptoms of seasonal allergies.[1][2] It is usually administered orally once a day. Montelukast is a CysLT1antagonist; it blocks the action of leukotriene D4 (and secondary ligands LTC4 and LTE4) on the cysteinyl leukotriene receptor CysLT1 in the lungs and bronchial tubes by binding to it. This reduces the bronchoconstriction otherwise caused by the leukotriene and results in less inflammation.
Because of its method of operation, it is not useful for the treatment of acute asthma attacks. Again because of its very specificmechanism of action, it does not interact with other asthma medications such as theophylline.
Another leukotriene receptor antagonist is zafirlukast (Accolate), taken twice daily. Zileuton (Zyflo), an asthma drug taken four times per day, blocks leukotriene synthesis by inhibiting 5-lipoxygenase, an enzyme of the eicosanoid synthesis pathway.
The Mont in Montelukast stands for Montreal, the place where Merck developed the drug.[3]
Singulair was covered by U.S. Patent No. 5,565,473[9] which expired on August 3, 2012.[10] The same day, the FDA approved several generic versions of montelukast.[11]
On May 28, 2009, the United States Patent and Trademark Office announced their decision to launch a reexamination of the patent covering Singulair. The decision to reexamine was driven by the discovery of references that were not included in the original patent application process. The references were submitted through Article One Partners, an online research community focused on finding literature relating to existing patents. The references included a scientific article produced by a Merck employee around the key ingredient of Singulair, and a previously filed patent in the same technology area.[12]
On December 17, 2009, the U.S. Patent and Trademark Office determined that the patent in question was valid based on the initial reexamination and new information provided.[13]
Montelukast is currently available in film coated tablet and orodispersible tablet formulations for once-daily administration, and also available as an oral granule formulation which is specifically designed for administration to paediatric patients.
Patent family US17493193A claims crystalline Montelukast sodium and processes for its preparation . Patents within this family are not considered to be a constraint to generic competition because the protected technology may possibly be circumvented by the synthesis and use of different molecular forms and/or salts. Patent family US33954901P relates to the specific marketed oral granule formulation of Montelukast.
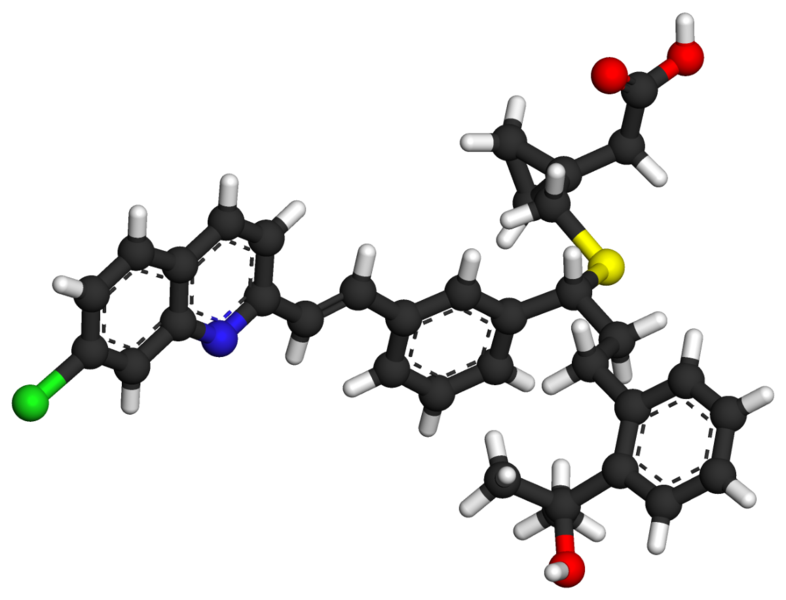
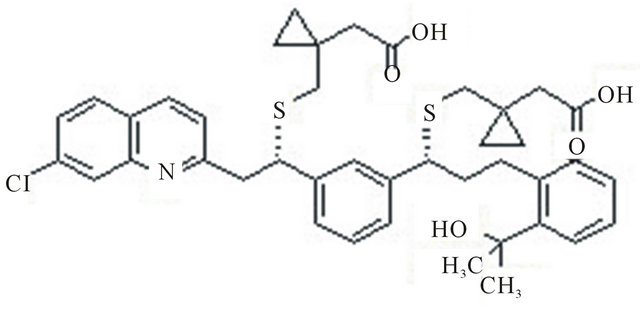
The chemical name of montelukast sodium is: Sodium 1-[[[(1R)-1-[3-[(1E)-2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl]cyclopropaneacetic acid and its structure is represented as follows:
Montelukast is apparently a selective, orally active leukotriene receptor antagonist that inhibits the cysteinyl leukotriene CysLT1 receptor.
The chemical name for montelukast sodium is [R-(E)]-1-[[[1-[3-[2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl] cyclopropaneacetic acid, monosodium salt. Montelukast sodium salt is understood to be represented by the following structural formula:
U.S. patent No. 5,565,473 (“‘473 patent”) is listed in the FDA’s Orange Book for montelukast sodium. The ‘473 patent recites a broad class of leulcotriene antagonists as “anti-asthmatic, anti-allergic, anti-inflammatory, and cycloprotective agents” represented by a generic chemical formula. ‘473 patent, col. 2,1. 3 to col. 4,1. 4. Montelukast is among the many compounds represented by that formula. The ‘473 patent also refers to pharmaceutical compositions of the class of leukotriene antagonists of that formula with pharmaceutically acceptable carriers. Id. at col. 10,11. 42-46.
Montelukast sodium is currently marketed by Merck in the form of film coated tablets and chewable tablets under the trade name Singular®. The film coated tablets reportedly contain montelukast sodium and the following inactive ingredients: microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, hydroxypropylcellulose, magnesium stearate, titanium dioxide, red ferric oxide, yellow ferric oxide, and carnauba wax. The chewable tablets reportedly containmontelukast sodium and the following inactive ingredients: mannitol, microcrystalline cellulose, hydroxypropylcellulose, red ferric oxide, croscarmellose sodium, cherry flavor, aspartame, and magnesium stearate. Physicians’ Desk Reference, 59th ed. (2005), p. 2141.
However, there is a need in the art to improve the stability of compositions of montelukast and particularly those of the sodium salt.
Montelukast sodium is a leukotriene antagonist and inhibits the leukotriene biosynthesis. It is a white to off-white powder that is freely soluble in methanol, ethanol, and water and practically insoluble in acetonitrile.
A montelukast sodium salt is a substance which exhibits efficacy of Singulair (available from Korean MSD) generally used for the treatment of asthma as well as for the symptoms associated with allergic rhinitis, which is pharmaceutically known as a leukotriene receptor antagonist. Leukotrienes produced in vivo by metabolic action of arachidonic acid include LTB4, LTC4, LTD4 and LTE4. Of these, LTC4, LTD4 and LTE4 are cysteinyl leukotrienes (CysLTs), which are clinically essential in that they exhibit pharmaceutical effects such as contraction of airway muscles and smooth muscles and promotion of secretion of bronchial mucus.
Montelukast sodium salt is a white and off-white powder which has physical and chemical properties that it is well soluble in ethanol, methanol and water and is practically insoluble in acetonitrile.
A conventionally known method for preparing a montelukast sodium salt is disclosed in EP Patent No. 480,717. However, the method in accordance with the EP Patent requires processes for introducing and then removing a tetrahydropyranyl (THP) protecting group and purification by chromatography, thus being disadvantageously unsuitable for mass-production. In addition, the method disadvantageously requires investment in high-cost equipment, for example, to obtain amorphous final compounds by lyophilization.
Meanwhile, U.S. Pat. No. 5,614,632 discloses an improved method for preparing a montelukast sodium salt by directly reacting a methanesulfonyl compound (2) with 1-(lithium mercaptomethyl)cyclopropaneacetic acid lithium salt, without using the tetrahydropyranyl protecting group used in EP Patent No. 480,717, purifying in the form of a dicyclohexylamine salt by adding dicyclohexylamine to the reaction solution, and converting the salt into a montelukast sodium salt (1).
However, the method in accordance with the US patent should use n-butyl lithium as a base in the process of preparing the 1-(lithium mercaptomethyl)cyclopropaneacetic acid lithium salt and thus requires an improved process due to drawbacks that n-butyl lithium is dangerous upon handling and is an expensive reagent.
PCT International Patent Laid-open No. WO 2005/105751 discloses a method for preparing a montelukast sodium salt, comprising coupling methyl 1-(mercaptomethyl)cyclopropane acetate (3) used in step 10 shown in Example 146 of EP Patent 480,717 with a methanesulfonyl compound (2) in the presence of a solvent/cosolvent/base, performing hydrolysis, recrystallizing the resultingmontelukast acid (4) in the presence of a variety of solvents to obtain highly puremontelukast acid (4), and converting the same into a montelukast sodium salt (1).
In addition, WO 2005/105751 claims that, in the coupling reaction, one is selected from tetrahydrofurane and dimethylcarbonate as a solvent, a highly polar solvent is selected from dimethylformamide, dimethylacetamide and N-methylpyrrolidone as a cosolvent, and one is selected from sodium hydroxide, lithium hydroxide, sodium hydride, sodium methoxide, potassium tert-butoxide, lithium diisopropylamine and quaternary ammonium salts, as a base.
However, WO 2005/105751 discloses that, since the coupling reaction requires use of a mixed solvent and the mixed solvent is different from the solvent used for hydrolysis, a process for removing the cosolvent through distillation under reduced pressure or extraction is further required prior to hydrolysis.
Further, in accordance with the method of WO 2005/105751, recrystallization is performed in the presence of a variety of solvents in order to obtain a highly puremontelukast acid (4) and the resulting recrystallization yield is varied in a range of 30 to 80%, depending on the solvent. In the case where desired purity is not obtained, recrystallization is repeated until montelukast acid (4) with a desired purity can be obtained. Disadvantageously, the method causes deterioration in overall yield.
European Patent No. 480,717 discloses montelukast sodium and its preparation starting with the hydrolysis of its ester derivative to the crude sodium salt, acidification of the crude to montelukast acid, and purification of the crude acid by column chromatography to give montelukast acid as an oil. The resulting crude oil in ethanol was converted to montelukast sodiumby the treatment with an equal molar aqueous sodium hydroxide solution. After removal of the ethanol, the montelukastsodium was dissolved in water and then freeze dried. The montelukast sodium thus obtained is of a hydrated amorphous form as depicted in FIG. 2.
The reported syntheses of montelukast sodium, as pointed out by the inventor in EP 737,186, are not suitable for large-scale production, and the product yields are low. Furthermore, the final products, as the sodium salts, were obtained as amorphous solid which are often not ideal for pharmaceutical formulation. Therefore, they discloses an efficient synthesis of montelukastsodium by the use of 2-(2-(3-(S)-(3-(7-chloro-2-quinolinyl)ethenyl)phenyl)-3-methanesulfonyloxypropyl)phenyl)-2-propanol to couple with the dilithium salt of 1-(mercaptomethyl)cyclopropaneacetic acid. The montelukast acid thus obtained is converted to the corresponding dicyclohexylamine salt and recrystallized from a mixture of toluene and acetonitrile to obtain crystallinemontelukast sodium. This process provides improved overall product yield, ease of scale-up, and the product sodium salt in crystalline form.
According to the process described in EP 737,186, the chemical as well as optical purities of montelukast sodium depends very much on the reaction conditions for the mesylation of the quinolinyl diol with methanesulfonyl chloride. For instance, the reaction temperature determinates the chemical purity of the resulting coupling product montelukast lithium, due to the fact that an increase in the reaction temperature resulted in decreased selectivity of mesylation toward the secondary alcohol. Mesylation of the tertiary alcohol occurred at higher temperature will produce, especially under acidic condition, the undesired elimination product, the styrene derivative. This styrene impurity is difficult to remove by the purification procedure using DCHA salt formation; while excess base, butyl lithium in this case, present in the reaction mixture causes the formation of a cyclization by-product, which will eventually reduce the product yield.
PCT WO 2005/105751 discloses an alternative process for preparing montelukast sodium by the coupling of the same mesylate as disclosed in ‘186 patent with 1-(mercaptomethyl)cyclopropane alkyl ester in the presence of a base. In this patent, the base butyl lithium, a dangerous and expensive reagent, is replaced with other milder organic or inorganic base. However, the problem concerning the formation of the styrene impurity is still not resolved.
Process for the manufacture of 1-[[[(1R)-1-[3-[(1E)-2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl]cyclopropane acetic acid, sodium salt [montelukast sodium (I)] consisting of: i. Converting methyl 1-(mercaptomethyl)-cyclopropaneacetate to a metal salt (X) using a metal hydroxide, ii. Subjecting the metal salt (X) to monometallation to provide a dimetallide (XI). iii. Converting a diol of formula (II) to a mesylate of formula (III) and reacting (III) in situ with (XI) affordin the metal salt of 1-[[[(1R)-1-[3-[(1E)-2-(7-chloro-2-quinolinyl)ethenyl]phenyl]-3-[2-(1-hydroxy-1-methylethyl)phenyl]propyl]thio]methyl]cyclopropane acetic acid. iv. Reacting the metal salt in-situ with a base and purifying to afford an amine salt (XII). v. Treating (XII) with a sodium base and precipitating out montelukast sodium (I).
more info
European Patent No. 480,717 disclose the montelukast and its preparation method first be hydrolyzed to the crude ester derivatives sodium, then this crude product was acidified to montelukast acid (montelukastacid), Finally, column chromatography purification of this crude acid into oily montelukast acid. This oilMontelukast acid in ethanol, by equimolar amounts of sodium hydroxide solution and converted to montelukast sodium. The ethanol was removed aftermontelukast sodium dissolved in water, followed by freeze-drying. Finally obtainedmontelukast shown in Figure 2 is amorphous hydrated.
The invention, in European Patent No. 737,186 points out, thismontelukast synthesis method is not suitable for mass production, and the low yield. Moreover, the resulting amorphous solid salt, are generally not used in pharmaceutical formulations. Therefore, they disclose the synthesis of an effective method of montelukast sodium, which uses 2 – (2 – (3 – (S) – (3 – (7 – chloro-2 – quinolinyl) ethenyl) phenyl) -3 – methylsulfonyl) phenyl) -2 – propanol and 1 – (methylthio alcohol) cyclopropane coupling the lithium salt of acetic acid, the resulting Montelukast acid is converted into a corresponding bicyclic hexyl amine salt, and from a mixture of toluene and acetonitrile recrystallization to prepare crystalline montelukast. This method greatly improves the productivity, ease of mass production, and the product is crystalline sodium salt.
According to European Patent No. 737,186 described method for preparingmontelukast chemical purity and optical purity depends largely quinoline diol with methanesulfonyl chloride in the reaction between the mesylated condition. For example, the reaction temperature resulted in an increase of the secondary alcohols methanesulfonyl selective reduction, the reaction temperature determines the coupling product (montelukast lithium) chemical purity. Occurs at a higher temperature mesylation tertiary alcohols, in particular under acidic conditions, will produce impurities, such as styrene derivatives. This impurity is difficult styrene generated by using the DCHA salt (DCHA salt formation) in the purification process to remove; present in the reaction mixture and excess base, butyl lithium cyclized by-products resulting in the formation will eventually reduce the yield of the product.
W02005/105751 disclose another preparation method of montelukast sodium, which is the methanesulfonic acid (European Patent No. 737,186 is the same) in an alkaline state where 1_ (methyl mercaptan yl) cyclopropyl alkyl ester and coupling thereof. In this patent, the dangerous and expensive alkaline-butyl lithium reagent, is replaced by other more moderate organic or inorganic base. However, the formation of styrene impurity problem is still not resolved
Lipkowitz, Myron A. and Navarra, Tova (2001) The Encyclopedia of Allergies (2nd ed.) Facts on File, New York, p. 178, ISBN 0-8160-4404-X
…………………….
Improved Process for the Preparation of Montelukast: Development of an Efficient Synthesis, Identification of Critical Impurities and Degradants
HPLC (isocratic mode) chromatograms were measured with the EliteLachrom device made by the Hitachi Company. Stationary phase: RP-18e was used for the analyses; column temperature was 20 °C. Mobile phase: Acetonitrile (80%) and a 0.1 M aqueous solution of ammonium formate adjusted to pH 3.6 with formic acid (20%) were used. The flow rate of the mobile phase was 1.5 mL/min. Detection at the wavelength of 234 nm was used. Methanol was used as the solvent for preparation of samples; 10−20 μL of the solution was used for the injection. The isocratic HPLC method was used for checking the compositions of the reaction mixtures. HPLC (gradient mode) chromatograms were measured with the Alliance HPLC device with PDA detector. Stationary phase: STAR RP-8e, 250 mm × 4 mm, 5 μm was used for the analyses; column temperature was 15 °C. Mobile phase: Acetonitrile (A) and 0.01 M aqueous solution of KH2PO4 adjusted to pH 2.2 with phosphoric acid (B) were used. Gradient mode with the flow rate of mobile phase 0.8 mL/min was used. Composition on the start was 60% of A and 40% of B, then changed to 15% of A and 85% of B over 20 min; this composition was held for 5 min, then changed to 60% of A and 40% of B over 5 min, and this composition was held to the end (overall time 35 min.). Detection at the wavelength of 234 nm was used. Methanol was used as the solvent for the preparation of the samples; 10−20 μL of the solution was used for the injection. The gradient HPLC method was used for checking the quality of the target substance including its salts with amines and of isolated standards of impurities. HPLC (determination of (S)-enantiomer by HPLC) chromatograms were measured with the Alliance HPLC device with PDA detector. Stationary phase: Chiralpak IA (5 μm), size 0.25 m, internal diameter 4.6 mm (manufactured by Daicel) was used for the analyses, column temperature 10 °C. Mobile phase: hexane/ethanol/1,4-dioxan/trifluoroacetic acid (77:3:20:0,1 v/v/v) was used. The flow rate of the mobile phase was 1.0 mL/min. Detection at the wavelength of 285 nm was used. Methanol was used as the solvent for preparation of samples; 10 μL of the solution was used for the injection. The isocratic elution was used for checking the optical purity of target montelukast. Typical retention times: montelukast: 9.3 min, (S)-montelukast: 12.9 min.
KEY REFERENCES
(a) Ray, U. K.;Boju, S.; Pathuri, S. R.; Meenakshisunderam, S. (Aurobindo Pharma Limited, India). PCT Patent Application WO/2008/001213, 2008.
(b) Wang, Y.; Wang, Y.; Brand, M.; Kaspi, J. (Chemagis Ltd., Israel). PCT Patent Application WO/2007/088545, 2007.
(c) Turchetta, S.;Tuozzi, A.; Ullucci, E.; de Ferra, L. (Chemi S.P.A.; Italy). European Patent Application EA 1,693,368, 2008.
(d) Srinivas, P. L.; Rao, D. R.; Kankan, R. N.; Relekar, J. P. (Cipla Limited, India). PCT Patent Application WO/2006/064269, 2006.
(e) Reguri, B. R.; Bollikonda, S.;Bulusu, V. V. N. C. S.; Kasturi, R. K.; Aavula, S. K. (Dr. Reddy’s Laboratory, India). U.S. Patent Application U.S.2005/0107612, 2005.
(f) Coppi, L.; Bartra Sanmarti, M.; Gasanz Guillen, Y.; Monsalvatje Llagostera, M.; Talavera Escasany, P. (Esteve Quimica, S.A., Spain). PCT Patent Application WO/2007/051828, 2007.
(g) Hung, J. T.; Wei, C. P. (Formosa Laboratories, Inc., Taiwan). U.S. Patent Application U.S.2008/0097104, 2008.
J. Liang*, J. Lalonde, B. Borup, V. Mitchell, E. Mundorff, N. Trinh, D. A. Kochrekar, R. N. Cherat, G. G. Pai
Codexis, Inc., Redwood City, USA and Arch PharmaLabs Limited, Mumbai, India
Development of a Biocatalytic Process as an Alternative to the (-)-DIP-Cl-Mediated Asymmetric Reduction of a Key Intermediate of Montelukast
Org. Process Res. Dev. 2010, 14: 193-198
Montelukast sodium (Singulair®) is a leukotriene receptor antagonist prescribed for the treatment of asthma and allergies. Workers at Codexis used directed evolution and high-throughput screening to engineer a robust and efficient ketoreductase enzyme (CDX-026) that accomplished the asymmetric reduction of ketone A, which is essentially water insoluble, at a loading of 100 g/L in the presence of ca. 70% organic solvents at 45 ˚C. The (S)-alcohol B was obtained in >95% yield in >99.9% ee and in >98.5% purity on a >500 mol scale.
The enzymatic reduction entails the reversible transfer of a hydride from isopropanol to the ketone A with concomitant formation of acetone. The reaction is driven to completion by the fortuitous crystallization of the monohydrate B. The four-step conversion of B into montelukast sodium is described in the Merck process patent (M. Bhupathy, D. R. Sidler, J. M. McNamara, R. P. Volante, J. J. Bergan US 6320052, 2001). This biocatalytic reduction is superior to the reduction of A with (-)-DIPCl previously used in the manufacture of montelukast
Auraptene has shown a remarkable effect in the prevention of degenerative diseases. Many studies have reported the effect of auraptene as a chemopreventative agent against cancers of liver, skin, tongue, esophagus, and colon in rodent models.[1] The effect in humans is not yet known.
Curini, M., Carvotto, G., Epifano, F. and Giannone, G. “Chemistry and Biological Activity of Natural and Synthetic Prenyloxycoumarins”(2006). Current Medicinal Chemistry, 13, 199-222.
Fever is one of the most common problems and there is not a single person who does not suffer from this in his life at least once. But in some people symptoms such as tingling sensation, temporary paralysis of legs and arms may appear after an attack of fever. These are the symptoms of Guillian Barre syndrome.
Brain and backbone are very important for the movement of the body. Nerves that control the movements are also very important as they carry the signals from brain to the muscles. Muscles move according to the signals brought by the muscles. If the nerves get damaged due to some problems, symptoms such as paralysis of legs and arms, tingling sensation, losing muscles movements etc are seen. Nerve disorders are usually found in diabetic patients and alcoholics. But these may sometime appear in people after a viral infection.
When symptoms of Guillian Barre syndrome appear, the patient should be taken to the Neurologist immediately. NCS test is prescribed for the patient and depending on the test results, Guillian Barre syndrome can be confirmed. Some other test may also be required to rule out other diseases that have the same symptoms.
Treatment for Guillian Barre syndrome
If nerve damage due to Guillian Barre is only minor, the condition can be improved with few injections and physiotherapy. Improvement can be observed in two to three months. But if the severity is more and if the patient finds breathing also difficult, he should be admitted into the ICU. The patient is given treatment with medicines for five days. Treatment for Guillian Barre syndrome is expensive. The dosage of the medicine is decided depending on the body weight of the patient. Medicines may cost between Rs. 2 lakhs to 3 lakhs.
There is alternative treatment for Guillian Barre syndrome for those who cannot bear the expense of medicines. It is called the Plasmapheresis procedure. This helps in preventing the condition of the patient from deteriorating further. In this procedure, patient’s blood is taken out and plasma is separated. Blood without plasma is again transfused into the patient’s body. If necessary, healthy plasma taken from donors is also given to the patient. But this treatment should begin immediately after Guillian Barre syndrome is confirmed for effective results. This treatment costs nearly Rs. 1 lakh and the patient should be given physiotherapy treatment for muscle movement.
With 11 treatments in Phase I trials, 8 in Phase II, and 13 in Phase III, Bayer has a strong pipeline.
By far the most interest currently, given that the latest reports came out October 21st, is riociguat (BAY 63-2521),
which has had good news from its ongoing Phase III clinical trials of the treatment for pulmonary arterial hypertension, also known as PAH. PAH is a progressive condition that overburdens the heart.
Trials indicate subjects had improved heart function and could better tolerate physical exercise. Patients on riociguat improved their walking distance by 36 meters on average, while those on placebo showed no improvement.
Professor Hossein Ardeschir Ghofrani of University Hospital Giessen, the principal investigator, was quite pleased with the results and explained the value of the measurement. “The six-minute walk distance test is a well-validated clinical measure in patients with PAH, and therefore, the results of the PATENT-1 trial are encouraging. . .These data from the PATENT study suggest that riociguat may be a potential treatment option both for patients who have never been treated for PAH as well as for those who have received prior treatment.”
Hossein A. Ghofrani Associate Professor of Internal Medicine, MD (University of Giessen) 1995 Research interests: pulmonary hypertension, ischaemia-reperfusion, experimental therapeutics, clinical trials
Bayer Accelerates Clinical Development of Promising New Drug Candidates
Five new molecular entities projected to enter Phase III by 2015 / Addressing unmet medical needs in the areas of oncology, cardiology, and women’s health / Initiation of further studies with recently launched products planned to add new treatment options
Leverkusen, October 8, 2013 – Following the recent commercial introduction of five new drugs to address the medical needs of patients with various diseases, Bayer is now accelerating the development of further five promising drug candidates which are currently undergoing phase I and II clinical studies. The company today announced that it plans to progress these five new highly innovative drug candidates in the areas of oncology, cardiology, and women’s health into phase III clinical studies by 2015.
“Our Pharma research and development has done a tremendous job of bringing five new products to the market offering physicians and patients new treatment alternatives for serious diseases”, said Bayer CEO Dr. Marijn Dekkers. “Following our mission statement ‘Science For A Better Life’, the five chosen further drug candidates all have the potential to impact the way diseases are treated for the benefit of patients.”
Bayer CEO Dr. Marijn Dekkers “Our research and development activities are strongly focused on areas where treatment options are not available today or where true breakthrough innovations are missing”, said Prof. Andreas Busch, member of the Bayer HealthCare Executive Committee and Head of Global Drug Discovery at Bayer HealthCare. “Our drug development pipeline holds a number of promising candidates which we want to bring to patients who need them urgently”, said Kemal Malik, member of the Bayer HealthCare Executive Committee, Chief Medical Officer and Head of Pharmaceutical Development at Bayer HealthCare. “Furthermore we are continuing to expand the range of indications for all our recently launched products Xarelto, Stivarga, Xofigo, Riociguat as well as Eylea and further refine the profile of these drugs in specific patient populations.”
The five mid-stage candidates have been selected for accelerated development based on positive “proof-of-concept” data from early clinical studies. Three of them are development compounds in the area of cardiology or the cardio-renal syndrome: Finerenone (BAY 94-8862) is a next generation oral, non-steroidal Mineralocorticoid Receptor antagonist which blocks the deleterious effects of aldosterone. Currently available steroidal MR antagonists have proven to be effective in reducing cardiovascular mortality in patients with heart failure but have significant side effects that limit their utilization. Finerenone is currently in clinical Phase IIb development for the treatment of worsening chronic heart failure, as well as diabetic nephropathy.
The second drug candidate in the area of cardiology is an oral soluble guanylate cyclase (sGC) stimulator (BAY 1021189). The start of a Phase IIb study in patients with worsening chronic heart failure is expected later this year.
For the cardio-renal syndrome, a Phase IIb program with the investigational new drug Molidustat (BAY 85-3934) is under initiation in patients with anemia associated with chronic kidney disease and/or end-stage renal disease. Molidustat is a novel inhibitor of hypoxia-inducible factor (HIF) prolyl hydroxylase (PH) which stimulates erythropoietin (EPO) production and the formation of red blood cells. Phase I data have shown that inhibition of HIF-PH by Molidustat results in an increase in endogenous production of EPO.
In oncology, Copanlisib (BAY 80-6946), a novel, oral phosphatidylinositol-3 kinases (PI3K) inhibitor, was selected for accelerated development. Copanlisib demonstrated a broad anti-tumor spectrum in preclinical tumor models and promising early clinical signals in a Phase I study in patients with follicular lymphoma. A Phase II study in patients with Non-Hodgkin’s lymphoma is currently ongoing.
Bayer has also made good progress in the development of new treatment options for patients with gynecological diseases: sPRM (BAY 1002670) is a novel oral progesterone receptor modulator that holds the promises of long-term treatment of patients with symptomatic uterine fibroids. Based on promising early clinical data the initiation of a Phase III study is planned for mid-2014.
Initiation of further studies with recently launched products Bayer has successfully launched five new pharmaceutical products, namely Xarelto™, Stivarga™, Xofigo™, Eylea™, and Riociguat, which has very recently been approved in Canada under the trade name Adempas™.
Xarelto has been approved globally for five indications across seven distinct areas of use, allowing doctors to treat patients in a greater variety of venous and arterial thromboembolic conditions than any other novel oral anticoagulant. The company continues to study the use of Xarelto for the treatment of further cardiovascular diseases. Ongoing clinical Phase III studies include COMPASS and COMMANDER-HF. The COMPASS study will assess the potential use of Xarelto in combination with aspirin, or as a single treatment to prevent major adverse cardiac events (MACE) in nearly 20,000 patients with atherosclerosis related to coronary or peripheral artery disease. The COMMANDER-HF study will evaluate the potential added benefit of Xarelto in combination with single or dual-antiplatelet therapy to help reduce the risk of death, heart attack and stroke in approximately 5,000 patients with chronic heart failure and coronary artery disease, following hospitalization for exacerbation of their heart failure. In order to answer medically relevant questions for specific patient populations Bayer has initiated a range of additional Xarelto studies in patients with atrial fibrillation (AF) undergoing percutaneous coronary intervention with stent placement (PIONEER-AF-PCI), cardioversion (X-VERT) or an AF ablation procedure (VENTURE-AF). As an extension to the Xarelto clinical trial programme, a number of real-world studies are designed to observe and further evaluate Xarelto in everyday clinical practice. These include the XAMOS study of more than 17,000 orthopaedic surgery patients, which confirmed the clinical value of oral, once-daily Xarelto in routine clinical practice in adults following orthopaedic surgery of the hip or knee. XANTUS is designed to collate data on real-world protection with Xarelto in over 6,000 adult patients in Europe with non-valvular AF at risk of stroke while XANAP is designed to collate data on real-world protection with Xarelto in over 5,000 adult patients in Europe and Asia with non-valvular AF at risk of stroke. XALIA will generate information from over 4,800 patients treated for an acute DVT with either Xarelto or standard of care.
In the area of oncology, Stivarga has been approved in 42 countries for use against metastatic colorectal cancer that is refractory to standard therapies, and additionally for gastrointestinal stromal tumor (GIST) in the US and Japan. Bayer is now planning to assess Stivarga in earlier stages of colorectal cancer as well as other cancer types. A Phase III trial in patients with colorectal cancer after resection of liver metastases is currently under initiation. Based on early clinical data Bayer has also initiated a Phase III study in liver cancer in patients who have progressed on sorafenib treatment.
Furthermore, the anti-cancer drug Xofigo (radium 223 dichloride) is a first-in-class alpha-pharmaceutical which is designed for use in prostate cancer patients with ‘bone metastases’ (secondary cancers in the bone) to treat the cancer in the bone and to help extend their lives. Xofigo is approved in the US for the treatment of patients with advanced castrate-resistant prostate cancer with symptomatic bone metastases. In addition, the European CHMP recently gave a positive opinion for radium 223 dichloride for the same use. The decision of the European Commission on the approval is expected in the fourth quarter of 2013. Based on the excellent Phase III results for Xofigo in patients with castration resistant prostate cancer and symptomatic bone metastases Bayer is looking to expand the use of Xofigo to earlier stages of the disease, and plans to initiate a Phase III study in combination with the novel anti-hormonal agent abiraterone. In addition, early stage signal-generating studies in other cancer forms where bone metastases are important causes of morbidity and mortality are planned.
In the area of pulmonary hypertension Adempas (Riociguat) is the first member of a novel class of compounds – so-called ‘soluble guanylate cyclase (sGC) stimulators’ – being investigated as a new and specific approach to treating different types of pulmonary hypertension (PH). Adempas has the potential to overcome a number of limitations of currently approved treatments for pulmonary arterial hypertension (PAH) and addresses the unmet medical need in patients with chronic thromboembolic pulmonary hypertension (CTEPH). It was approved for the treatment of CTEPH in Canada in September 2013, making it the world’s first drug approved in this deadly disease. Riociguat has already shown promise as a potential treatment option beyond these two PH indications. An early clinical study was conducted in PH-ILD (interstitial lung disease), a disease characterized by lung tissue scarring (fibrosis) or lung inflammation which can lead to pulmonary hypertension, and, based on positive data, the decision was taken to initiate Phase IIb studies in PH-IIP (idiopathic pulmonary fibrosis), a subgroup of PH-ILD. Moreover, scientific evidence was demonstrated in preclinical models that the activity may even go beyond vascular relaxation. To prove the hypothesis Bayer is initiating clinical studies in the indication of systemic sclerosis (SSc), an orphan chronic autoimmune disease of the connective tissue affecting several organs and associated with high morbidity and mortality. If successful, Riociguat has the potential to become the first approved treatment for this devastating disease.
In the area of ophthalmology, Eylea (aflibercept solution for injection) is already approved in Europe and several additional countries for the treatment of neovascular (wet) age-related macular degeneration and for macular edema following central retinal vein occlusion. In September, Bayer HealthCare and Regeneron Pharmaceuticals presented data of the two phase III clinical trials VIVID-DME and VISTA-DME of VEGF Trap-Eye for the treatment of diabetic macular edema (DME) at the annual meeting of the Retina Society in Los Angeles and at the EURetina Congress in Hamburg, Germany. Both trials achieved the primary endpoint of significantly greater improvements in best-corrected visual acuity from baseline compared to laser photocoagulation at 52 weeks. Bayer plans to submit an application for marketing approval for the treatment of DME in Europe in 2013.
About Bayer HealthCare The Bayer Group is a global enterprise with core competencies in the fields of health care, agriculture and high-tech materials. Bayer HealthCare, a subgroup of Bayer AG with annual sales of EUR 18.6 billion (2012), is one of the world’s leading, innovative companies in the healthcare and medical products industry and is based in Leverkusen, Germany. The company combines the global activities of the Animal Health, Consumer Care, Medical Care and Pharmaceuticals divisions. Bayer HealthCare’s aim is to discover, develop, manufacture and market products that will improve human and animal health worldwide. Bayer HealthCare has a global workforce of 54,900 employees (Dec 31, 2012) and is represented in more than 100 countries. More information at www.healthcare.bayer.com.
a stock market blog that provides free stock market analysis. A piece entitled “Pfizer: Alzheimer’s Drugs Will Carry Stock To New Highs In 2013” had a subheading “strong pipeline.”
Turns out that was too optimistic, as Pfizer’s Alzheimer’s drug–along with Johnson and Johnson’s–both failed to produce. But many stock analysts still hold hope that Pfizer has a new ‘cash cow’ coming down the pipeline.
notes that Pfizer currently has 87 drugs in its pipeline. While its true that most are in the early stages, 11 are ready to be reviewed by the FDA.
That number puts it ahead of most of its rivals, with Eli Lilly, a close second, having 63 drugs in Phases 1-3, plus one currently being reviewed. Bristol-Myers Squibb has 46 drugs in development, 7 under review, Merck has 35 drugs in Phase 2 or 3 with two under review, and Johnson and Johnson has 18 drugs that are already in Phase 3 clinical trials or up for FDA approval.
But, of course, as the journal points out, “Quality trumps quantity. . . . One or two blockbusters can be better than several lower-revenue drugs.”
So what does Pfizer have up its sleeve that might begin to fill the very big shoes of Lipitor?
Well, the company has diversified the therapeutic areas under research, with 26% of R&D efforts going toward oncology treatments, 20% to neuroscience and pain, 17% to cardiovascular and metabolic diseases, 14% to inflammation and immunology, 5% to vaccines, and 18% toward ‘other.’
Pfizer has several medicines for diabetes alone coming up, in Phase I and Phase II trials, almost all meant to treat type 2 diabetes.
its blockbuster potential in this area is limited by the existing treatments of Merck and Sanofi. 10% of Sanofi’s total sales come from Lantus,
a diabetes drug useful for both types 1 and 2, and Merck made $1.3 billion off its Januvia
franchise in the first quarter of this year alone.
So hopes are pinned on Pfizer’s tofacitinib, currently under FDA review, as the treatment with the potential to earn $1 billion or more in sales, easing the gaping wound left by Lipitor. Tofacitinib prompts such high hopes because it might possibly treat rheumatoid arthritis, psoriasis, and irritable bowel syndrome. Some analysts have pinned this as the cash cow Pfizer so badly needs to replace treatments lost to the patent cliff.
If it gets approved, Tofacitinib would be first treatment for rheumatoid arthritis (RA) in a new class of medicines (known as Jenus kinase, or JAK, inhibitors), and the first JAK inhibitor approved for rheumatoid arthritis.
Tofacitinib showed statistically significant improvement compared to placebo in decreasing the symptoms of RA (as measured by 20% improvement in the American College of Rheumatology scale), in improving physical function (as measured by mean change in Health Assessment Questionnaire-Disability Index), and in leading to remission (as measured by Disease Activity Score 28 ESR).
Joel Kremer, MD, chief of medicine at Albany Medical College in N.Y., after analyzing the data, commented, “Tofacitinib appears to reduce the signs and symptoms of rheumatoid arthritis very quickly. We hope that after carefully considering the benefit/risk equation, this compound will provide an additional valuable treatment option for patients who have experienced inadequate response to prior treatments.”
Pfizer also believes its blood thinner Eliquis, which it is developing with Bristol-Myers Squibb (see below) could be a big money-maker.
ViiV Healthcare, a joint venture involving GlaxoSmithKline (GSK), Pfizer and Shionogi, has submitted a New Drug Application (NDA) to the US Food and Drug Administration (FDA) for its investigational single-tablet regimen (STR) combining dolutegravir, abacavir and lamivudine for treatment of HIV-1 patients.
Ranbaxy Laboratories has secured approval from India’s Central Drugs Standard Control Organisation (CDSCO) to produce and market its Synriam drug in the country to treat malaria caused by the Plasmodium vivax parasite in adults.
AltheRx Pharmaceuticals has received a notice of allowance for its patent application from the US Patent and Trademark Office (USPTO) for the use of solabegron, a beta 3-adrenergic receptor agonist, in combination with antimuscarinics at both therapeutic and sub-therapeutic doses, for the treatment of overactive bladder (OAB).
Solabegron was discovered by GlaxoSmithKline and acquired by AltheRx in March 2011. Solabegron relaxes the bladder smooth muscle by stimulating beta-3 adrenoceptors, a novel mechanism compared to older established drug treatments for overactive bladder syndrome such as the anticholinergic agents. Astellas Pharma have developed the first commercially available β3 adrenergic receptor, mirabegron, which is now licensed in Japan[6] and the US[7] for overactive bladder. Mirabegron is not licensed for irritable bowel syndrome.
A Phase II study of Solabegron for overactive bladder (OAB) looked at 258 patients with moderate to severe incontinence experiencing an average of 4.5 wet episodes per day. Results demonstrated a statistically significant improvement with Solabegron as compared to placebo, as measured by the percent reduction of the number of wet episodes and the absolute number of daily voids.
A Phase II study for irritable bowel syndrome (IBS) evaluated 102 patients with IBS. Solabegron demonstrated significant reduction in pain associated with the disorder and a trend for greater improvement in the quality of life, compared to placebo.
Both Phase II studies indicated a tolerability profile for Solabegron that was similar to placebo. The OAB patients did not suffer from dry mouth, constipation, increase in heart rate or cognitive issues.
AltheRx is currently preparing to advance Solabegron into a large clinical study in OAB.
Synthesis
Hicks A, McCafferty GP, Riedel E, Aiyar N, Pullen M, Evans C, Luce TD, Coatney RW, Rivera GC, Westfall TD, Hieble JP. GW427353 (solabegron), a novel, selective beta3-adrenergic receptor agonist, evokes bladder relaxation and increases micturition reflex threshold in the dog. Journal of Pharmacology and Experimental Therapeutics. 2007 Oct;323(1):202-9.doi:10.1124/jpet.107.125757PMID 17626794
Grudell AB, Camilleri M, Jensen KL, Foxx-Orenstein AE, Burton DD, Ryks MD, Baxter KL, Cox DS, Dukes GE, Kelleher DL, Zinsmeister AR. Dose-response effect of a beta3-adrenergic receptor agonist, solabegron, on gastrointestinal transit, bowel function, and somatostatin levels in health.American Journal of Physiology. Gastrointestinal and Liver Physiology. 2008 May;294(5):G1114-9. PMID 18372395
Kelleher DL, Hicks KJ, Cox DS, et al. Randomized, double-blind, placebo (PLA)-controlled, crossover study to evaluate efficacy and safety of the beta 3-adrenergic receptor agonist solabegron (SOL) in patients with irritable bowel syndrome (IBS). Neurogastroenterol Motil 2008;20 (Suppl 2):131.
Cellek S, Thangiah R, Bassil AK, Campbell CA, Gray KM, Stretton JL, Lalude O, Vivekanandan S, Wheeldon A, Winchester WJ, Sanger GJ, Schemann M, Lee K. Demonstration of functional neuronal beta3-adrenoceptors within the enteric nervous system. Gastroenterology. 2007 Jul;133(1):175-83.
Schemann M, Hafsi N, Michel K, Kober OI, Wollmann J, Li Q, Zeller F, Langer R, Lee K, Cellek S. The beta3-adrenoceptor agonist GW427353 (solabegron) decreases excitability of human enteric neurons via release of somatostatin.Gastroenterology 2009 Sep 25. [Epub ahead of print]



































 Copper-based radiopharmaceuticals for diagnostic imaging can target the amyloid-β plaques implicated in Alzheimer’s disease
Copper-based radiopharmaceuticals for diagnostic imaging can target the amyloid-β plaques implicated in Alzheimer’s disease